Published March 25, 2026 10:40AM
Yoga Journal’s archives series is a curated collection of articles originally published in past issues beginning in 1975. This article first appeared in the March-April 1996 issue of Yoga Journal.
The human neuroendocrine system has changed very little since the time of cave people. Yet today we are likely to receive more stimulation in one day than our ancestors did in their entire lifetime. Beginning with the “alarm” clock in the morning and ending with the drive through “rush” hour traffic, our bodies face an extraordinary level of stimulation and acceleration. It shouldn’t surprise us that heart disease is rampant, high blood pressure epidemic, and autoimmune diseases on the rise as we propel ourselves at ever increasing speeds toward the new millennium.
One of the first things that happens when we respond to a stressful situation is a change in our breathing.
Stress may be real or imagined—an important distinction for us to remember, but not one that the nervous system itself makes. Just imagining a stressful event can reduce inhalation volume. When we have been exposed to continual stress over a period of time—whether in the form of marathon running or divorce court proceedings—the body can literally forget how to relax.
The stage is set for a habituated stress response that keeps us tense regardless of whether we have any reason to be so. How we breathe may become more a statement about what happened to us in the past than what is happening to us in the present.
Contrary to popular belief, there is no one correct way to breathe. But there are specific and common ways that people restrict their breathing. When we obstruct our breathing, we cut ourselves off from the most accessible and readily renewable source of energy a human being has. When our respiratory process is freed, we breathe in a way that is fitting for each situation.
Our breathing spontaneously responds to changes in activity, body position, temperature, noise, and, of course, stress.
While pranayama (yogic breathing exercises) can be used to strengthen and refine breathing, many of us practice pranayama without addressing underlying breath-holding habits. Paradoxically, the manipulation and control of the breath used in pranayama is frequently employed to suppress the deep-seated tears and insecurities that cause holding patterns in the first place.
It was only after I stopped practicing pranayama that I was able to determine the ways in which I controlled and obstructed my breathing process. The process of dismantling these holding patterns allowed me to make a direct and honest encounter with the feelings and forces that lay beneath them.
Learning how to breathe well is thus not an additive process in which we learn specific techniques for improving our breathing. It is a process of deconstruction, in which we learn to identify and let go of the things we are already doing that restrict the natural emergence of the breath.
How can you tell if your breathing is disordered or restricted? You may already sense you are not breathing as fully as you could. You may feel out of breath or notice that your breathing is erratic, labored, or shallow. You may even see a link between your breathing and your low energy, chronic anxiety, or other health conditions.
In this article (drawn from my upcoming book, The Breathing Book, published by Henry Holt), we’ll look at some of the common ways that people restrict their breathing—and explore ways that these restrictions can be released. Before we look at some of the common breath-holding patterns, it’s important to know how you are currently breathing so you can compare and appreciate changes that may occur during and after some of your breathwork. Checking in with your breathing should be done briefly, because the moment you observe your breathing you are likely to try to change it.
Checking In With Your Breathing
Sit in a comfortable chair with your back upright and your feet firmly planted on the floor. You may want to have a friend observe you and makes notes to give you a more objective assessment. (If you are a helping partner, refrain from offering psychological interpretations of your observations, which can undermine confidence.) Sit for a moment and sense your breathing. As you ask yourself the following questions, wait for your reactions to come through. Don’t worry if your impressions are vague or blurry—this is a normal stage most people will go through. Over time the sensations will become more specific and defined.
Where do I feel my breathing?
Place one hand on your abdomen and one hand on your upper chest. Can you feel where the breath originates? Let your perceptions come through without editing or analyzing them.
Don’t discount small movements or seemingly insignificant perceptions. Do you feel particular areas of your body where the breath is more noticeable? In your abdomen, chest, or nostrils? Around the ribs? Do you notice your breathing around your shoulders or breastbone
What does my breathing feel like?
What is the quality of your breathing? Is it rough, labored, jerky, rhythmic? Does it feel smooth or mechanical? Let any words or images arise. You may want to make a note of them for future reference.
How fast do I breathe?
Without trying to alter your breathing in any way, count the number of times you breathe in and out per minute when you are sitting quietly. An inhalation and an exhalation equals one breath cycle. Because you will probably try to correct your breathing by slowing it down, you might ask a close friend or partner to surreptitiously gauge your breaths per minute.

Sensing the Diaphragm
All breath-holding patterns involve a partial contraction of the diaphragm. The diaphragm is the central most important muscle for breathing. It is a parachute-shaped structure with the top of the dome lying just underneath the heart and the sides and front attaching to the inner rib cage and the tip of the breast bone.
In the back of the dome there are long muscles called crura which insert along the front of the spinal column and act as anchors for the parachute. In healthy breathing the diaphragm moves without restriction, descending as we inhale and ascending as we exhale (Figure 1). Do the following inquiry before you proceed to the breath-holding patterns.
Inquiry: Contracting Your Diaphragm
Purpose: This inquiry is designed to help you feel how your diaphragm responds to stress. It will help you to identify when you are contracting and restricting the free movement of this muscle.
Here’s how: You can do this inquiry sitting, standing, or lying down. Place one hand on your upper abdomen just below the base of your sternum. Relax the muscles in your body and feel the free movement of the diaphragm under your hand as you breathe. Because the diaphragm lies deep in your body, you will be sensing the referred movement on the surface of the body. With a quick and strong action, clench the fist of your other hand. Did you feel the diaphragm “jump” under your hand? Did you feel that it clenched just like your hand? Experiment with suddenly contracting any part of your body, even your toes, and you will find that any sudden or strong contraction in your outer muscles echoes back immediately to your inner breathing muscles. When the outer muscles of the body ready themselves for action, the inner muscles follow suit.
Common Breath-Holding Patterns
Now that you have a general impression of your breathing, you can look at some of the specific ways that you restrict or limit it. The patterns presented here are by no means comprehensive (as each person’s breathing is as unique as a finger print) but they demonstrate some of the most common ways people interfere with their breathing. For the sake of clarity, I focus on the more extreme manifestation of each pattern, but the patterns can exist in varying degrees. (In other words, you need not be an emergency room candidate in a panic attack to be a hyperventilator; like me, you may simply tend to breathe too fast most of the time.)
Before you read through the description of each pattern, pause and check in with your own breathing. As you read on, sense whether your own breathing resembles the pattern. Do the descriptions resonate with you? Try imitating the particular breathing pattern that is described. Does it feel familiar or unfamiliar? Remember that your breathing may resemble more than one of the breath patterns outlined.

1. Reverse Breathing
What it looks like: In correct breathing, the diaphragm descends during inhalation and the downward pressure causes the abdomen to billow outwards.
When we breathe out, the diaphragm moves up into the chest causing a slight drawing inwards and upwards through the abdomen. In reverse breathing, the abdomen moves in on the inhalation (Figure 2) and out on the exhalation, although the person may never allow the abdomen to completely relax at any phase of the breath. This is a reversal of the natural rhythm of the breathing movement. This kind of breathing often arises from the habit of wearing restrictive clothing or tight belts, which make it impossible for the abdomen to expand during any phase of the breath.
What it does to the body/mind: Reverse breathing causes a kind of confusion in the diaphragm and all the muscles of respiration, as well as confusion and a sense of disorientation in the mind. You may experience chronic tension in your upper body, especially around the back of the neck, upper shoulder, upper back, and jaw area. You may also suffer from indigestion, heart burn, bloating, flatulence, or a feeling of a lump in the throat.
Often reverse breathers encounter great difficulty learning body movements, feeling clumsy and uncoordinated because their most basic pattern of movement (breathing) is completely upside down. Reverse breathers get particularly confused when asked to breathe in or out during a particular phase of a movement. They also may have no sense of when they are breathing in and when they are breathing out.
To test yourself: Take a moment and watch the movement of your breath down the front of your body. Looking at your body rather than feeling your body is helpful because reverse breathers can rarely feel what they are doing. See if you can identify the movements in your body when you breathe in and out.
Dismantling the pattern:
- Relax your abdomen. Experiment with consciously allowing the abdomen to move out on your inhalation and in on your exhalation. You don’t need to push the abdomen out or pull it in mechanically. Simply let it happen and observe how it feels to experience your breathing in this way.
- Slow down so you can become more aware of the reversal in your breathing pattern.
2. Chest Breathing or Paradoxical Breathing
What it looks like: Chest breathing, which is also known as “paradoxical breathing,” is a naturally occurring reflex that happens when we are suddenly startled or frightened (as when someone jumps out at us).
We gasp, pull the abdomen in, and breathe high into the chest. The lift of the abdomen and pelvic floor prevent the diaphragm from descending completely as we inhale. Unable to get the air we need, we may fight even harder on the next breath to suck the breath in. The harder we try the less air we get.
Chest breathers restrict the movement of the breath in the abdomen, forcing the breath higher up into the chest (Figure 3). Chest breathing is usually accompanied by the shoulders moving up and down, and even during exhalation the shoulders may stay tense. Breathing into your chest is not necessarily pathological; in full body breathing you will see the chest and shoulders and the entire body move slightly on the inhalation. In full body breathing, however, breathing is experienced as a simultaneous and global sensation throughout the body. This opening is not achieved as a result of suppressing movement somewhere else.
What it does to the body/mind: When we chest breathe, we use our secondary or accessory respiratory muscles instead of the primary muscles. In efficient breathing, we rely primarily on the diaphragm (the massive bellows of the body), the intercostals (the muscles in between the ribs), and the abdominals. When these muscles are doing their job, the accessory muscles in the upper chest and neck such as the pectoralis, trapezius, and scalenes are relatively passive. A chest breather will rely almost entirely on these weak upper body muscles and thus develop chronic tension in the thoracic spine, shoulders, and neck. This tension is usually resistant to therapy such as massage or body work, because the tension is recapitulated as soon as the person resumes chest breathing—that is, 22,000 times a day!
Chest breathers favor expansion of their upper lungs. Although chest breathing looks impressive, it is actually a very inefficient form of breathing. Bringing air into the lower lungs creates a more efficient exchange of oxygen due to the higher density of blood capillaries in the lower lobes of the lung.
Because the abdominal muscles are chronically tightened, all the organs in the lower body suffer from a lack of circulation. Ironically, this person may be holding the abdomen in as a strategy for looking thin, but the healthy functioning of the organs of digestion, assimilation, and elimination is so seriously impaired that weight loss measures may be fruitless.
When we chest breathe, we prevent the diaphragm from descending completely on the inhalation. Because we can’t breathe in fully, we also can’t breathe out fully. As a result we may resort to breathing more quickly to make up for the lack of oxygen. This sets the stage for a breath-holding pattern that is even more serious hyperventilation.
Chest breathers are often associated with type-A personalities, the kind of people who sit on the edge of their seats and exude anticipation in their entire bearing. These people never seem to have enough time to do all the tasks they have set themselves. Chest breathers often experience a chronic, free-floating state of anxiety. After all, this is the way we breathe during a stress reaction. There is now strong scientific evidence that shows a correlation between chest breathing and a higher incidence of heart disease and high blood pressure.
Chest-breathing is the most common breathing disorder of our culture. As you become more aware of this pattern, you may start to notice just how many people breathe this stress-filled way.
To test yourself: Put one hand on your abdomen and place the other hand on your chest, on and above the sternum. Which moves more? Feel whether the abdomen expands fully, billowing outward as you breathe in. Or do you feel yourself pulling upward and inward with your abdomen? One way to gauge this is by noting whether you feel increased tension in your shoulders when you breathe in. Do your shoulders rise with the incoming breath rather than broadening out to the sides? If both chest and abdomen move simultaneously, you are probably not a chest breather. Remember, a chest breather suppresses the breath lower down, forcing it to move higher up into the body.
Dismantling the pattern:
- Release and relax your shoulders and upper back.
- Experiment with consciously allowing the abdomen to move out on your inhalation and in on your exhalation. You don’t need to push the abdomen out or pull it in mechanically. Let it happen. So that you can expand your abdomen when you breathe, consider throwing away (or giving away) tight fitting clothes, restrictive belts, and clothes that are too small for you.
- Assess your body image. Do you harbor unrealistic expectations about your body?
- Ground yourself in the present. Be aware of when your mind is racing into the future.
3. Hyperventilation
What it looks like: Hyperventilation is not usually recognized except in its extreme form, but it can be both subtle and chronic. When you are sitting quietly, your breathing rate should be about 13 breaths per minute (BPM), according to Dr. Robert Fried, author of The Breath Connection (Insight Books). Men usually breathe a little slower (12 to 14 BPM) and women usually breathe a little faster (14 to 15 BPM). When we develop the habit of hyperventilating, we breathe quickly regardless of what we are doing, and our body reacts in dramatic ways to this change. This type of breathing is the natural consequence of chest breathing and has all the symptoms of that pattern.
Most restrictive breathing patterns involve a partial contraction of the diaphragm. When the diaphragm cannot descend completely during inhalation, it reduces the space in the chest that the lungs can expand into. With this limited lung capacity, less oxygen is taken in with each breath. Most people will compensate for this lack of oxygen by increasing the number of breaths they take per minute.
What it does to the body/mind: The first thing that happens when we hyperventilate is that we lose too much carbon dioxide (COz) from the body. While most of us know that the body needs oxygen for survival, you may be surprised to find out that we also need carbon dioxide. Carbon dioxide is the crucial ingredient in helping us maintain the right acid-alkaline balance of the blood (about pH 7.40). The slightest changes in the pH of the body can cause marked alterations in the rates of chemical reactions in the cells, some slowing down and others speeding up. When the body loses too much carbon dioxide the metabolism shifts from acid to alkaline.
According to research by Dr. Robert Fried, when CO2 decreases below normal levels (and alkalinity increases), the following systems are affected:
- Brain arteries: The arteries in the brain constrict, reducing the blood flow and hence the delivery of oxygen to the brain tissues. (Common symptoms: headache, lack of concentration)
- Hemoglobin and oxygen retention: Hemoglobin, the molecule in your red blood cells that carries oxygen, will now tend to retain oxygen rather than giving it up to the tissues. This may perpetuate the hyperventilation pattern as the body continues to get less oxygen than it needs. (Common symptoms: dizziness, feeling of breathlessness)
- Body arteries: The arteries in the body constrict, resulting in reduced blood flow to the extremities in the body. (Common symptoms: cold hands and feet)
- Muscles and nerves: The increase in alkalinity causes an increase in the amount of calcium entering muscles and nerves, making them hyperactive. (Common symptoms: muscle tension)
- Nervous system: Low levels of carbon dioxide generally result in increased excitability of the nervous system. The nerves may become so excitable that they automatically and repetitively fire even when they are not receiving normal stimulation to do so. (Common symptoms: rushed interactions, inappropriate responses, overreaction to minor problems)
In 1978 the Journal of the American Medical Association produced a list of conditions that were thought to be related to hyperventilation. They included but were not limited to: fatigue, exhaustion, heart palpitations, rapid pulse, dizziness and visual disturbances, numbness and tingling in the limbs, shortness of breath, yawning, chest pain, a feeling of a lump in the throat, stomach pain, muscle pains, cramps and stiffness, anxiety, insomnia and nightmares, impairment of concentration and memory, and—not surprisingly—a feeling of “losing one’s mind.”
To test yourself: Try lifting your abdomen in and up and breathing high into your chest. Your breastbone will move up and down without any lateral expansion. Does this feel familiar or unfamiliar to you?
Counting the number of breaths you take in a minute may give you a rough idea of whether you hyperventilate but has limited accuracy because of the likelihood that you will try to slow your breathing down. A more helpful approach is to take “glances” of your breathing throughout the day and sense if you are breathing more quickly than you really need to for the activity that you are doing. You may be surprised to discover that your breath rate may be accelerated in the most sedentary activities.
Other clues: Do you allow your exhalation to reach its full completion or do you rush for the next breath? Do you fail to allow a brief pause at the end of the exhalation? Do you pull the inhalation into the body rather than letting it stream in of its own accord? These are all signs that your breathing is faster than it needs to be. You may also sigh or yawn frequently to make up for your otherwise shallow breathing.
Dismantling the pattern:
- Follow the tips for Chest Breathing.
- Focus on increasing your exhalation.
- “Deaccelerate” some of your activities. Your breathing will mirror the rate at which you do things. Try driving your car more slowly. Write some of your letters long hand at the end of the day instead of typing them. Can you think of other activities that you normally speed up through mechanization that you could do (at least some of the time) without the acceleration?
- Incorporate some menial work into every day. Any task that is repetitive and involves slow rhythmic body movement will help replace your breathing. Try shoveling in the garden, sewing or knitting, kneading bread, folding laundry or ironing, chopping vegetables. As your breathing slows to match the rhythm of the activity, you will find the mind entering a calm and peaceful state.
- If you are hyperventilating because you are rushing to complete a job or task, consider these questions: Is my need to hurry real or imagined? Is this task so important that it is worth the loss of my peace of mind? and, the clincher, Will anyone die as a result of this not getting done today?
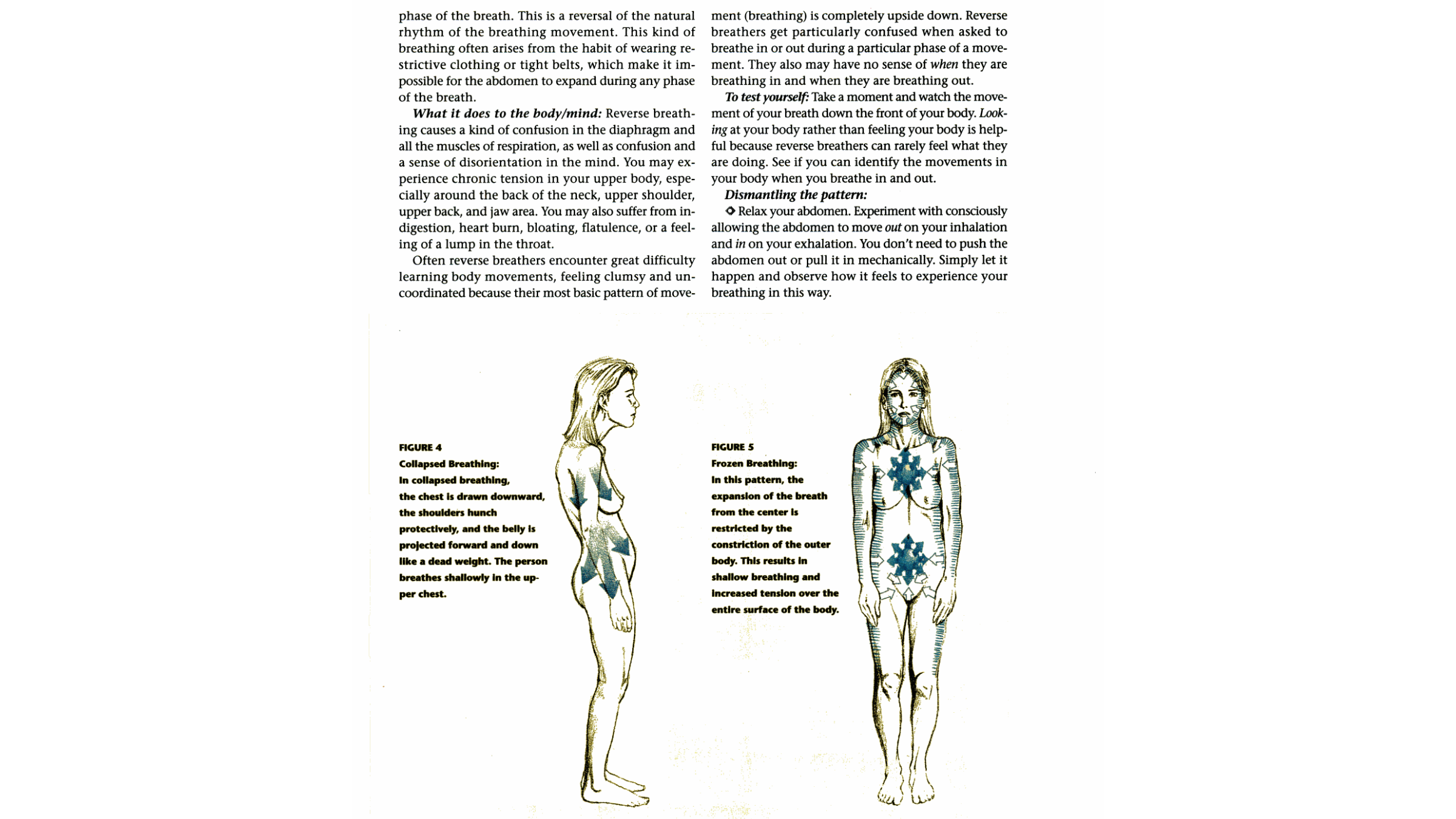
4. Collapsed Breathing
What it looks like: Collapsed breathers (Figure 4) are basically chest breathers with an entirely different posture and approach. Because I personally tend to chest breathe through lifting up, it wasn’t clear to me that one could chest breathe as a result of collapsing downward until I observed this pattern in others. In chest breathing caused by abdominal holding, the whole body moves up; in collapsed breathing, the whole body moves downward. The chest is drawn downward, the shoulders hunch protectively, and the belly is projected forward and down like a dead weight. In this pattern there is too little tone in the lower body—not just in the abdominal muscles, but in the abdominal organs themselves. The soft organs in the belly appear to be bloated and stagnant, while the heart and lungs press listlessly down upon the belly. I frequently see this pattern in obese persons and in people suffering from depression.
In this pattern the belly remains relatively static, as the upper chest and shoulders make half-hearted puffs up and down. The sound of the exhalation is often like a contained sigh. Collapsed breathers sigh and gasp frequently in an attempt to get more air.
What it does to the body/mind: In collapsed breathing there is often an intense disassociation from the body. We may be ashamed of how our body looks, or we feel so uncomfortable in our body that we exist outside its boundaries. We may have grown up believing that the body is simply an apparatus for carrying the head, and as a result we disconnected ourselves from any sensation below the neck. On the opposite end of the spectrum, collapsed breathing may be the result of harboring terrible memories of past trauma, where numbing and checking out were the primary strategies for surviving. These strategies may very well have been the best (and perhaps only) way we could cope with terrible circumstances, but the continuation of the pattern leaves us disconnected from ourselves and disconnected from present sources of aliveness. Depression and a sense of life being a burden may be our daily wake-up call.
It is not unusual to meet people with this breathing pattern who are very lively individuals—but only from the neck up. They live in the world of ideas, often in the world of business, where the body is seen to be of little use—an object that gets exercised if there is any time left at the end of the work day. I have listened to people with this pattern speak with great animation in their faces and eyes while the body itself does not reflect or express itself either through movement or gesticulation.
To test yourself: Put one hand on your chest and one hand on your belly while you are sitting. Exaggerate collapsing the chest downward, letting the head come forward and the breastbone downward. At the same time let the belly protrude outwards. Now press down through your feet and allow the chest to lift, opening up the space around the middle of your body. Feel the belly come alive as there is an upward lift through the central organs. Notice if the first pattern feels comfortable and familiar to you and whether the second feels strange and unfamiliar. If you feel uncomfortable opening the abdomen and letting the chest lift, your muscles are probably very unused to carrying you in this way, and it is likely that you are a collapsed breather.
Dismantling the pattern:
Unlike many of the other breath holding patterns, the solution to collapsed breathing lies in increasing rather than decreasing the tone in the body.
The focus should be on opening the center of the body. In collapsed breathing, the body weight descends into the ground and is compressed by the force of gravity. By pressing into the ground with the feet, whether sitting or standing, you can create a rebounding force that lifts and elongates you through your central axis. Some of my students call this action the “body kabob,” because it feels like a skewer straightening the body out. This internal lift also creates a psychological lift, helping us to meet the day with greater optimism and hope.
- If you found the previous exercise in opening the chest emotionally uncomfortable and you feel very disconnected or numb in your body, you may want to seek the help of a compassionate therapist. Whatever feelings lie dormant within you will most certainly surface if you begin to open your body, and for this reason it would be wise to seek guidance so you can contain the retrieval process in a way that feels safe for you.
5. Breath Grabbing
Our breath rhythm has three parts: the exhalation, the pause, and the inhalation. In her book Ways to Better Breathing (Healing Arts Press), Carola Speads says that “the pause fulfills a double purpose: a resting from the effort of the inhalation and a rallying of the energy needed for the next inhalation. The pause, therefore, is not an idle period when nothing is happening; it is a vital phase in the breathing process…. If we interfere with the length of the breathing pause, shortening it even slightly, we find ourselves feeling ‘rushed’ and ‘pressured,’ that well-known state that interferes so often with our sense of well-being and is such a generally acknowledged burden in our daily lives.”
“Breath grabbers” grasp for the next breath without allowing the pause to take its natural course. Breath grabbers are often the kind of people who finish other peoples sentences for them. They may also be uncomfortable allowing for pauses or silence within a conversation. We have all had the experience of jumping in on the tail end of someone else’s sentence or even cutting into the last few words to launch our own monologue.
(New Yorkers seem to be famous for this kind of fast repartee, while jokes are often made about folks from the midwest who allow for cavernous pauses between words.) Breath grabbers often feel that if they don’t jump in and reach for what they want, they’ll miss out, be left out, or be left behind.
Allowing for pauses does not mean we mechanically prolong the natural pause. You can’t make a pause happen. It comes as a natural result of learning to relax into the breath and trusting that you don’t need to grasp for something that will come on its own accord. A deep, abiding sense of ease, surrender, and relaxation will arise when you allow yourself to drink in the peace of this pause.
Dismantling the pattern:
- Practice letting other people finish their sentences, and allow for a pause before you speak. Observe your breathing as you listen to others.
- Is there room in your life for pauses? If not, can you restructure your time? Can you say no to new projects and responsibilities or delegate tasks to others so you have more time to smell the roses?
- Pause on cues that you assign yourself, such as a ringing phone or a glimpse of your favorite color. When cued, pause and feel the moment in between your inhalation and your exhalation.
6. Frozen Breathing
You may have noticed that on a very cold day you brace yourself by contracting muscles throughout your body. When you contract your muscles, you are actually breathing very shallowly.
In frozen breathing (Figure 5), the entire outer layer of the body contracts to constrict and suppress the rising movements of the breath, much like a snake might squeeze its prey. When we breathe freely, the inner soft organs and the outer musculoskeletal system move with one another. In frozen breathing the outer container remains rigid. Very little movement is seen on the surface of the body, and the body appears “frozen.” This pattern is very common in people who are aggressively goal oriented.
“Getting there” always supersedes “being here.” These people will hold their breaths in order to balance in a yoga pose, get the dinner on the table in time, or meet a work deadline. Frozen breathers will often rationalize their tension by saying “when I’m finished with this project, or as soon as this is over… then I’ll relax!” The root of this pattern is fear—fear of not being good enough, fear of not getting there, and fear of not becoming someone.
Surprisingly, this is a very common breath-holding pattern in yoga practitioners. While practicing yoga, a frozen breather does not allow the relaxation to be communicated through the tissue during exhalation. The muscles stay hard and the shoulder, elbow, and knee joints are often locked. The entire focus is on attaining the “final” position rather than experiencing the immediate sensations of the pose.
Frozen breathing can also be a consequence of having lived in great fear for an extended period of time. In this case, the posture is more characteristic of someone cringing or drawing away suspiciously. Children who have been physically or sexually abused, veterans suffering post-traumatic shock syndrome, and others who have lived through devastating experiences may freeze their body and breath as a way of coping with overwhelming feelings. A yoga teacher working with such a person must develop his trust and confidence and work gently and gradually to “warm” the breathing process. Teachers can build confidence through encouragement and through consistently affirming the student’s improvements rather than focusing on their weaknesses. In this way the student learns to trust that he has the capacity to change.
Dismantling the pattern:
- Frozen breathers need to focus on softening and releasing the tightness in their muscles. Yoga, tai chi, dancing, and massage are excellent body practices for these people.
- If you feel that your breathing pattern is the result of unresolved feelings from the past, consider finding a therapist who can offer support and guidance to you.
Dismantling Breath-Holding Patterns
Most breathing patterns are the accumulation of a lifetime’s experience and are as familiar to us as our way of walking. The nervous system has become conditioned to repeat these patterns even when the patterns are dysfunctional.
Dismantling your own breath-holding patterns involves a number of simple steps. The first step is to identify what you do in your body when you restrict your breath. The second step is to identify when you hold your breath. The third step is to disengage from the holding pattern—that is, relax any unnecessary tension, then allow the breath to emerge by itself. The last step is to reinforce good breathing habits by creating optimal conditions—that is, by cultivating a flexible, strong, and relaxed body so that breathing well can become an integral part of who you are.
Rather than asking yourself what you can do to open your breathing, ask yourself what you are already doing and how this may be interfering with free breathing. Also consider some of the unconscious forces that may be driving your breathing habits and how those forces affect your daily choices. For instance, if it is more important to you to look good than to feel good, you have already made a choice about the quality of life that will be available to you.
While we may have thrown out the girdles and corsets of our forebears, we may still be wearing a psychic girdle as we constantly measure ourselves on the finicky scale of the culture at large. This psychological girdle is far more damaging and powerful than any girdle we could wear, because most of the time we don’t know we are wearing it and we never take it off.
When you do notice yourself holding tension in key areas such as the throat, abdomen, pelvic floor, or shoulders, consciously relax and release these tight areas on an exhalation. Try exaggerating the tension for seven seconds, then releasing it, to clarify the difference between tension and relaxation.
Most people are quick to jump to the conclusion that their breath holding patterns will be corrected quickly through doing breathing exercises or through trying to “breathe deeper.” Not so. If we walk with a limp it is likely that we will run with a limp, and so it is with breathing. If our everyday breathing pattern is distorted, it is most likely that we will attempt to do breathing exercises with the same underlying tensions and compensations. Entering the process of identifying and dismantling our personal breath-holding patterns requires courage, honesty, and a willingness to proceed patiently. Also beware of having such eagerness to “untie” your breathing that you pull and tug on yourself, much as you might pull on the links of a knotted chain, and in doing so unwittingly increase the tension in your breathing. If you can be patient, you will find that the breath will magically open to you in the same way that a knotted chain falls open when you play with it patiently. There is very little between you and the magic of this opening.
This article is a compilation of extracts from The Breathing Book by Donna Farhi (Henry Holt, 1996). The Breathing Book contains a wide selection of inquiries that explore how to breathe and support the emergence of a more natural breath pattern.




{kind=link}